
Are Race Scholars Paranoid?
March 19, 2026Are Race Scholars Paranoid?
March 19, 2026The Obesity-Diabetes Hoax
More than 75% of “obese” Americans DO NOT have diabetes. And the story only gets stranger from there.
I had planned a lunch n’ Zoom with one of my girlfriends recently. We’ll call her Tess. Tess happens to be one of the most recognizable faces in the fat liberation space.
I tossed crushed red pepper onto my store-bought pizza and logged on. When our Zoom chat connected, I was surprised to see two faces. She was there as planned, eating fettuccini, but there was another woman sitting next to her.
“This is my intern, Elena.” Elena and I exchanged hellos.
“Elena just arrived from Ukraine.” Tess informed me.
“Oh wow!” I exclaimed. I tried to think of something non-triggering to say. All I could muster was, “Well, welcome.”
“Thanks.” She replied flatly.
“I’m kind of surprised you could even get into the US right now, what with all the chaos.”
“Yah. Everyone says that.” Elena said. “I’m lucky because I got here before the Public Charge rule. Otherwise maybe I’d be denied entry for ‘obesity.’” She explained.
“WHUT?” I exploded. Nearly spitting pizza shards. “Fat people can’t come into America now?!”
“Oh yeah girl, you didn’t hear?” Tess replied. “Yah, back in November Trump issued a new Public Charge rule that requires people applying for visas to be screened for the likelihood of becoming a social liability. And now 'obesity' is a medical condition that may be considered in the application process.” She stopped to wind pasta around her fork.
“May be?” I probed.
“They want to give consular officials the latitude to discriminate.” She explained.
I was blown to smithereens.

I wasn’t shocked by the callousness. That’s the reason I don’t follow Trump-related news in the first place. I was shocked that they’d somehow orchestrated a legal basis to discriminate on the basis of size. And if you know anything about fatphobia, you’ll know that the people it targets are overwhelmingly BIPOC and under-resourced. Immigrants to the US largely come from countries with significant populations from each of these groups. Now, these potential immigrants had to undergo a visual inspection from a doctor who could, acting on their own discretion, claim an immigrant is too fat for entry to the USA. Another diabolical way to deny entry to non-wealthy, non-white folks the Trump admin considers undesirable.
But how much truth is there to the claim that being fat is a sickness? We’ve already covered the problem of BMI as a tool of measurement. Now, let’s consider the case of the supposed link between elevations in BMI, and the #1 medical condition it has been associated with: Type 2 diabetes.
The relationship is supposedly so strong that there’s a term for it: Diabesity. And don’t think medical professionals are shy about throwing it around either.
But is it a real thing? Is it true that having a BMI ≥ 30 means that you are destined to develop adult-onset diabetes?
* * *
You’ve heard the argument before. People with higher BMIs have higher rates of diabetes. Therefore, obesity is a “primary risk factor” for diabetes. The folks promoting this idea imply causation without saying it. Or proving it.
From there, the rhetoric tends to escalate quickly—talk of epidemics, of a generation at risk, of bodies as ticking time bombs. The fat people, the story goes, are just so sick. The assumption is so widespread that it has quietly become the scaffolding for all sorts of public policy, including immigration policy. But that scaffolding, it turns out, is shakier than it looks.
Here’s the long and short of it: If a BMI ≥ 30 had a clear, strong, and straightforward connection to diabetes, medical and other policy professionals might just have a smoking gun on their hands to thrust right in your face.
So, let’s try and find it. It’s a simple question: what percentage of people with a BMI of 30 or greater actually have diabetes? By now, hundreds if not thousands of studies must have demonstrated that X percent of people with a BMI above 30 are diabetic. What’s the magic number?!
I went hunting for that number and realized it did not exist.
Turns out, most studies do not report diabetes prevalence specifically within “obese” populations. That struck me as odd, because if they’re trying to frighten us about the connection between big bodies and diabetes, they’ll want to give us that clear, incontrovertible number.
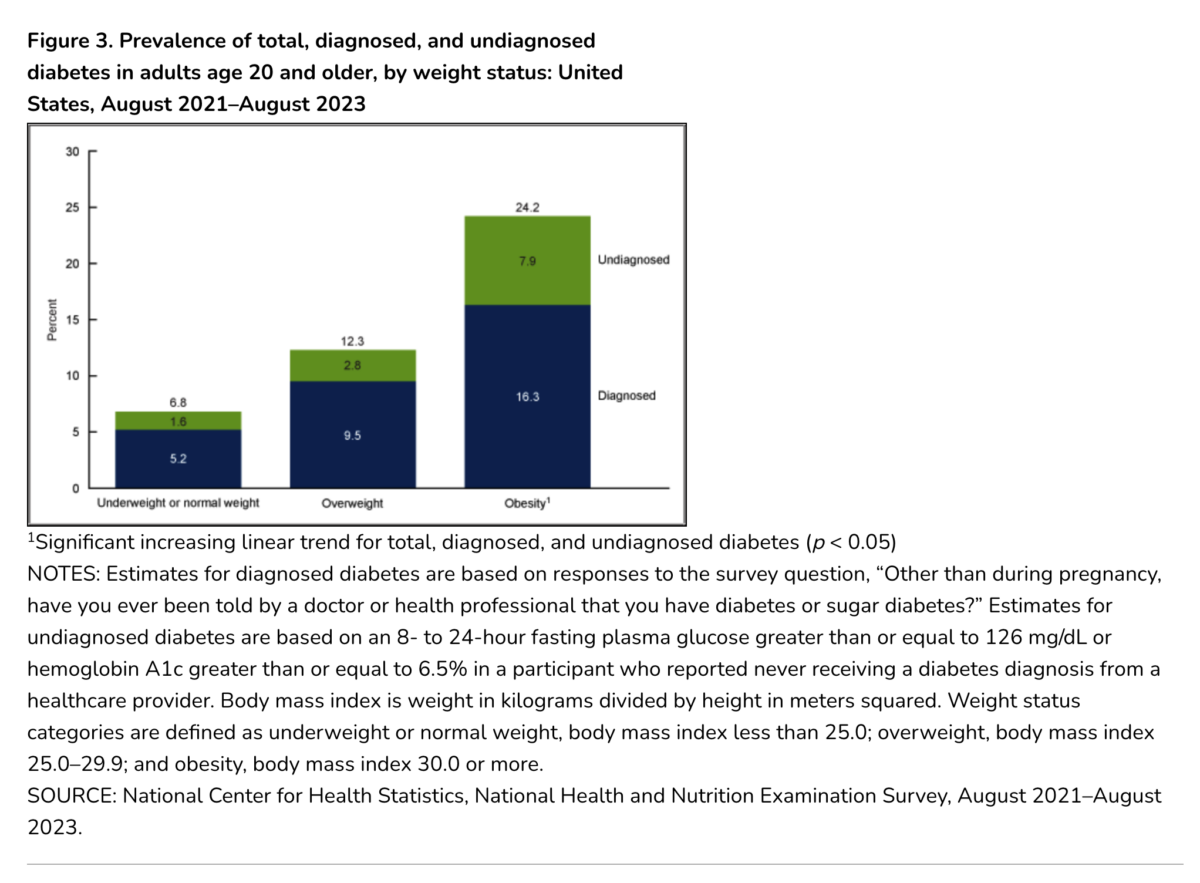
What I found is that in the U.S. among people considered obese, according to the CDC, 24% have diabetes. That’s higher than the supposed “normal weight” population, whose rate is about 7%. If being labeled obese means a person has slightly less than a 1 in 4 chance of developing diabetes, that’s not nothing. But it is, nevertheless, clearly a relatively unlikely outcome. It means over 75% of “obese” people WILL NOT have diabetes.
Even this number, this 24%, is not rock solid. I’ve seen other estimates suggesting somewhere between 14-43% of American “obese” people have diabetes, which is an insane amount of variability. In statistics speak, this is called “substantial heterogeneity,” or better yet, “low reliability.” In other words, the relationship between BMI and diabetes is not reliable.
Alright. I lowkey already knew that. I am a medical sociologist after all. I’ve published multiple papers on the link between BMI and diabetes. Back in 2023, myself and two amazing public health scholars published a paper showing that the correlation between BMI and diabetes varied significantly by race/ethnicity.
But, for the purposes of this piece, I wanted to know more. I wondered, even though the relationship between weight and type 2 diabetes (T2D) varies widely in the U.S., do we find a similar pattern of variability in other countries?
In the U.S., about 11% of people are diabetic, and supposedly 43% of adults are obese. This is a population ratio of diabetes to obesity (DO) that is about 1:4. For every one diabetic, there are nearly four people considered obese. In Canada, that ratio is about 10% to 33% or 1:3.3. In England it’s about 10% to 27%, or 1.2.7. Have you noticed that the one thing remaining nearly static is the rate of diabetes across these countries? All nearly 10%. But notice how widely the prevalence of “obesity” varies. The connection between diabetes and “obesity” varies markedly by country. Hmm!
Let’s get into the juicy bits. We'll jump out of the West and into the East. In China, about 10% of adults have diabetes, just like in the Western countries we’ve been discussing. Their “obesity” rate? About 15%. That means their ratio is 1:1.5. That’s nearly 1:1. Are we to believe that nearly every “obese” person in China is diabetic? But somehow in the USA less than ¼ of obese people are diabetic? Why should that be so??
Now, let me blow your mind. (drum roll please!)
In Japan, diabetes prevalence is an estimated 8.1%. Their “obesity” prevalence? 4%. Y’all, their rate of obesity is nearly half that of diabetes! How can obesity drive diabetes when the diabetes prevalence is twice that of obesity?
The same goes for India. Here we have one of the most populous nations on the planet. We are talking about nearly 1.5 billion people. About 11% are diabetic, 6% of the population has a BMI ≥ 30. Again, that’s a ratio of nearly 2:1. With the diabetes rate being nearly double that of obesity. Hot damn!
In case you need to see it, here’s that graphically:
|
Country |
Diabetes (%) |
Obesity (%) |
D:O Ratio |
|---|---|---|---|
|
|
11 |
43 |
1:4 |
|
|
10 |
33 |
1:3.3 |
|
|
10 |
27 |
1:2.7 |
|
|
10 |
15 |
1:1.5 |
|
|
8.1 |
4 |
2:1 |
|
|
11 |
6 |
~2:1 |






Notice that in every country, the diabetes rate is about the same. But! The “obesity” rate varies widely. How can obesity drive diabetes given these data?
I have to tell you about something über f*ed up I found out about when researching this. There’s a panic that the tide of obesity is rising in India. But guess what. You’ll never guess. Oooooohhh!! They are using a lower cutoff for obesity diagnosis to make this claim. Even though the BMI ≥ 30 is a bogus standard, it was adopted by the WHO as a planetary standard. But, in India they lowered it to between 23-27 (true story! read here!) and are now ginning up fear using a wholly different standard than the one applied to most of the world. Can you believe the insidiousness? (In case you are wondering, I used the global standard throughout this piece.)
* * *
Now let’s jump back to Trump’s policy. According to Google, these are the nations sending the most immigrants in recent years: Mexico, India, Venezuela, Cuba, Colombia.
Here’s the chart of the relationship between diabetes and “obesity” for these countries:
|
Country |
Diabetes (%) |
Obesity (%) (BMI ≥30) |
D:O Ratio |
|---|---|---|---|
|
|
15–17 |
30–31 |
~1:2 |
|
|
~10 |
~25–31 |
~1:2.5–3 |
|
|
~9–13 |
~18–22 |
~1:2 |
|
|
~9–10 |
~20–24 |
~1:2–2.5 |
|
|
~7–10 |
~20–25 |
~1:2–3 |
|
|
~9–11 |
5–7 |
~2:1 |





You might notice that the relationship between diabetes and elevated BMIs is much tighter for Latin and South America than the US, much less India (where the “primary risk factor” language simply does not apply). That could mean people from these countries will be particularly scrutinized by this law.
* * *
My bad. I set out to write something uplifting. “Diabesity” is a hoax. If the relationship between elevated BMI and diabetes is not only highly volatile, but in the case of Japan and India, reversed from that of many other countries, then obesity cannot be a cause of diabetes.
But, I did show who this policy might target and how. And this is why it’s critical for all of us to see the interrelationship among our struggles. Racial discrimination, fat discrimination, and immigration policy are deeply intertwined. All of this gives us plenty of good reasons to plot, plan, and organize together.